TO START |
W2I2P4E | Wash your hands Wear appropriate PPE Introduce yourself and check patient’s Identity (full name, DOB) Permission: “May I examine your abdomen?” Privacy: Ensure curtains to the bay are closed Pain: “Are you in any pain at all?” - if so where? Position: Start with the patient on the bed at 45o, then lie the patient flat to examine the abdomen Exposure: From the xiphisternum to the pubic symphysis (bra left on)
|
INSPECTION |
Surroundings | Monitoring – fluid balance Treatments – O2, IV infusions (note what and how much), total parenteral nutrition (TPN), NG tubes, surgical drains (note volume and colour of liquid draining), catheter (note volume), patient-controlled analgesia Paraphernalia – food and drink, Ensure, Creon (pancreatic insufficiency), nil by mouth signs, vomit bowl, stoma kit, cigarettes
|
Patient | Appearance - alert, confused (hepatic encephalopathy) Behaviour - writhing (colicky pain) very still (peritonism) Body habitus - obese, cachectic, abdominal distension (ascites) Colour - pallor (anaemia), jaundice, hyperpigmentation (haemochromatosis, Addison’s)
|
UPPER PERIPHERIES |
Nails | Clubbing (4Cs: Cirrhosis, Crohn’s, ulcerative Colitis, Coeliac) - look for Schamroth’s window Koilonychia - spoon-shaped nails (iron deficiency anaemia) Leukonychia - whitening of nail bed (low albumin: coeliac, cirrhosis, nephrosis)
|
Hands | Palmar erythema - redness of heel of the palm (chronic liver disease) Dupuytren’s contracture (associated with excess alcohol use) Tar stains (smoking increases risk of oesophageal and colon Ca, Crohn’s and peptic ulcers)
|
Arms | Asterixis - coarse flapping tremor when arms held out straight and wrists dorsiflexed for 15s (hepatic encephalopathy or ureaemia) Radial pulse - assess rate and rhythm Assess temperature Inspect for bruising (deranged clotting 2o to liver disease), excoriations (pruritis 2o to hyperbilirubinaemia), tattoos/track marks (risk factors for hepatitis) Offer to measure BP
|
Face | Eyes - conjunctival pallor (anaemia), scleral icterus (yellowing of the sclera; jaundice), Kaiser-Fleisher rings (copper deposits in iris seen with slit lamp; Wilson’s disease), xanthelasma, corneal arcus (hypercholesterolaemia) Mouth - oral candidiasis (immunosuppression), aphthous ulcers (Crohn’s, iron/B12/folate deficiency), angular stomatitis (fissuring of corners of mouth; iron/B12/folate deficiency), glossitis (beefy red tongue; iron/B12/folate deficiency) Breath - alcohol, pear drops (DKA), foetor hepaticus (liver failure) Bilateral parotid swelling (chronic alcohol abuse, recurrent vomiting eg. bulimia)
|
Neck | Lymphadenopathy - palpate for lymphadenopathy, esp in left supraclavicular fossa (Virchow’s node - drains lymph from abdomen, can be first sign of Ca, esp gastric, Troisier’s sign)
|
Chest | Inspect the chest for: Spider naevi - central red papule with fine lines radiating, >5 pathological (liver cirrhosis) Gynaecomastia - breast tissue in men, due to + oestrogen eg in liver cirrhosis Hair loss - due to + oestrogen
|
ABDOMEN |
Screening tests | Lie the patient flat Ask the patient to take a deep breath - pain/reduced movement suggests peritonism Ask the patient to lift their head to their chest - inspect for divarication of recti or paraumbilical/incisional hernia Ask the patient to cough while your hands are over the inguinal region - palpate for a hernia
|
Inspect | Distension (6Fs: fat, fluid, flatus, faeces, foetus or f***ing big tumour) Scars (see page 62): How old is the scar? Has it healed well? PEG tube Stomas - comment on position, spout, contents of bag Ileostomy (Usually RIF, spouted, green liquid) Colostomy (Usually LIF, flushed to skin, faeculent solid) Urostomy (RIF, spouted, contains urine)
Striae - stretch marks (pregnancy, Cushing’s – purple) Caput medusae - engorged paraumbilical veins (portal hypertension, liver cirrhosis) Grey-Turner sign - bruising around flanks (haemorrhagic pancreatitis) Cullen’s sign - bruising around the umbilical area (haemorrhagic pancreatitis) Pulsations (AAA)
|
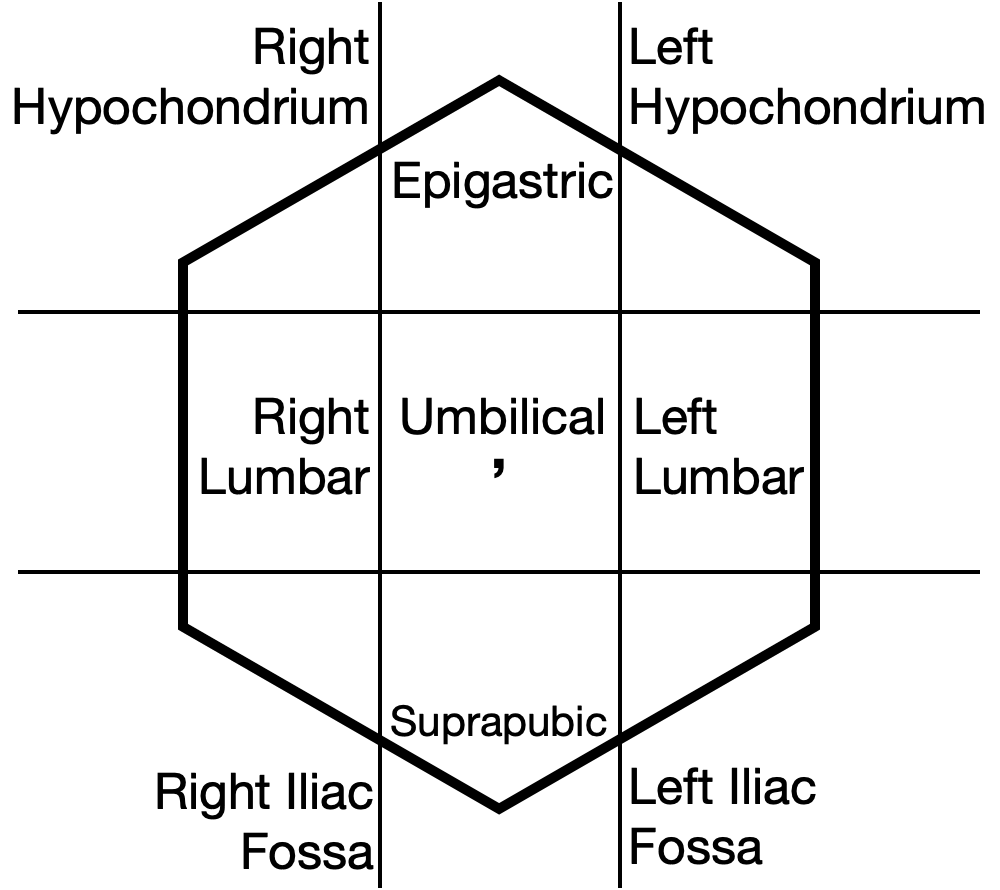
Palpate | Palpate the nine areas - first superficially, then deeply Look specifically for: Masses - see below Tenderness - note the area, rebound tenderness (peritonitis), Rovsing’s sign (palpating LIF causing pain in RIF; appendicitis) Guarding - abdominal muscle contraction on palpation, may be voluntary and distractible or involuntary (peritonism)
Palpate for organomegaly: Liver - ask the patient to take slow deep breaths in and out and palpate upwards from the RIF to R hypochondrium with the edge of your hand, palpating on inspiration - if enlarged will feel tap on inspiration (1-2cm below costal margin is normal) Hepatomegaly differential: chronic liver disease, cancers, R heart failure, lymphoma, leukaemia, sarcoid, amyloidosis
Spleen: Palpate from RIF to L hypochondrium as above (spleen should not be palpable in healthy individuals) Splenomegaly differential: lymphoma, leukaemia, portal hypertension, infection, sarcoid, amyloidosis
Ballot the kidneys: Place one hand in the patient’s flank and one hand anteriorly on their abdomen ‘Ballot’ the kidney from your hand on the patients back into your hand palpating their stomach - the kidneys are not usually palpable (unless low BMI)
Feel for the aorta: Using both hands, deeply palpate just superiorly to the umbilicus A normal aorta is palpable as a pulsatile mass An expansile mass suggests an AAA
Consider assessing for Murphy’s signs - palpation in the R hypochondrium and the patient taking a deep breath in causes the patient to wince with a ‘catch’ in breath due to pain, suggests cholecystitis
|
Percuss | Percuss: Liver for organomegaly - from RIF to R hypochondrium Spleen for organomegaly - from RIF to L hypochondrium Bladder for distention - downwards from umbilicus to suprapubic region Shifting dullness - to assess ++ ascites Percuss from the patient’s umbilicus to their L side If dull (suggesting fluid) ask the patient to roll towards you whilst keeping your hand on the area that was dull Percuss again after 30s - if resonant the dullness has shifted and suggests the presence of fluid in the abdomen
|
Auscultate | Bowel sounds - normal: gurgling, tinkling suggests obstruction, absent: suggests ileus Bruits - listen at renal arteries (superior and lateral to umbilicus) and aorta for bruits, suggestive of turbulent blood flow eg AAA, stenosis
|
LOWER PERIPHERIES |
Legs | Assess for peripheral oedema - note the level Erythema nodosum - red, tender nodules on shin, suggestive of Crohn’s
|
CLOSURE |
Closure | |
To complete (HIDE in the PUB) | Examine the Hernial orifices, Inguinal lymph nodes, Digital rectal examination (DRE) and External genitalia Pregnancy test (if female), Urine dip, Basic Obs (sats, BP, temp)
|