Arterial Blood Gas Interpretation
Arterial blood gas (ABG) measurement is a quick and handy way to identify chemical abnormalities such as problems with gas exchange, acid-base balance and electrolyte derangements in the blood that aid in analysing a clinical picture - remember that the background history and examination of a patient can provide useful clues for the interpretation of ABGs!
- Assess Oxygenation - should be >10kPa on room air. Always note the FiO2 (what % oxygen they’re on); as a rule of thumb, PaO2 ≈ FiO2 - 10. Clinical context is important here - a patient may only be sustaining a ‘normal’ PaO2 through supplemental oxygen or hyperventilation!If the patient is hypoxic, assess PaCO2 to determine the type of respiratory failure:
- ↓PaO2 without ↑PaCO2 = Type 1 Respiratory Failure (gas exchange problem: O2 unable to get in but more soluble CO2 can still diffuse out)
- ↓PaO2 with ↑PaCO2 = Type 2 Respiratory Failure (ventilation problem: alveolar air is not being replenished hence no O2 entering or CO2 leaving)
- Determine Acid-Base Status - Acidosis is pH <7.35 and Alkalosis is pH >7.45
- Is it a respiratory problem?
- If pH <7.35 and the PaCO2 >6.0kPa – respiratory acidosis
- If pH >7.45 and the PaCO2 <4.7kPa – respiratory alkalosis
OR
Is it a metabolic problem?
- If pH <7.35 and the HCO3- (bicarbonate) < 22mmol/L – metabolic acidosis
- If pH >7.45 and the HCO3- (bicarbonate) > 26mmol/L – metabolic alkalosis
- BE > 2 = metabolic alkalosis
- BE <-2 = metabolic acidosis
Alternatively, base excess measures the concentration of acid/base that must be added to the sample to return it to pH 7.4 corrected for PaCO2, i.e. isolating the metabolic component
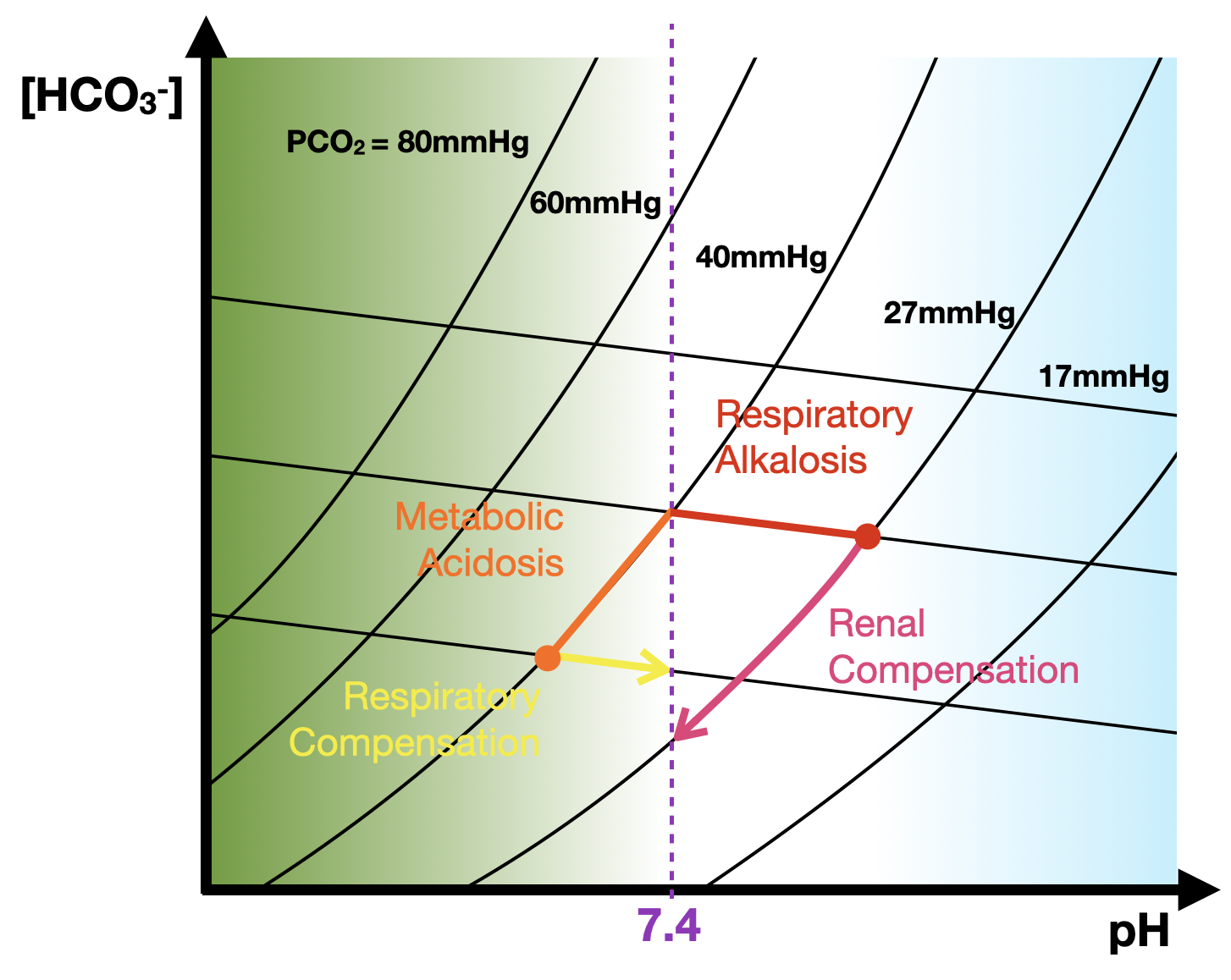
- Are there compensatory changes?
- Respiratory compensation (hypo/hyperventilation) occurs in minutes-hours
- i.e. ↑pCO2 in metabolic alkalosis and ↓pCO2 in metabolic acidosis
- Metabolic compensation (by kidneys) occurs in hours-days
- i.e. ↑HCO3- in respiratory acidosis and ↓HCO3- in respiratory alkalosis
- If there is metabolic acidosis, where is the acid coming from?
- A drop in HCO3- is sometimes a consequence, rather than the primary cause, of a metabolic acidosis.
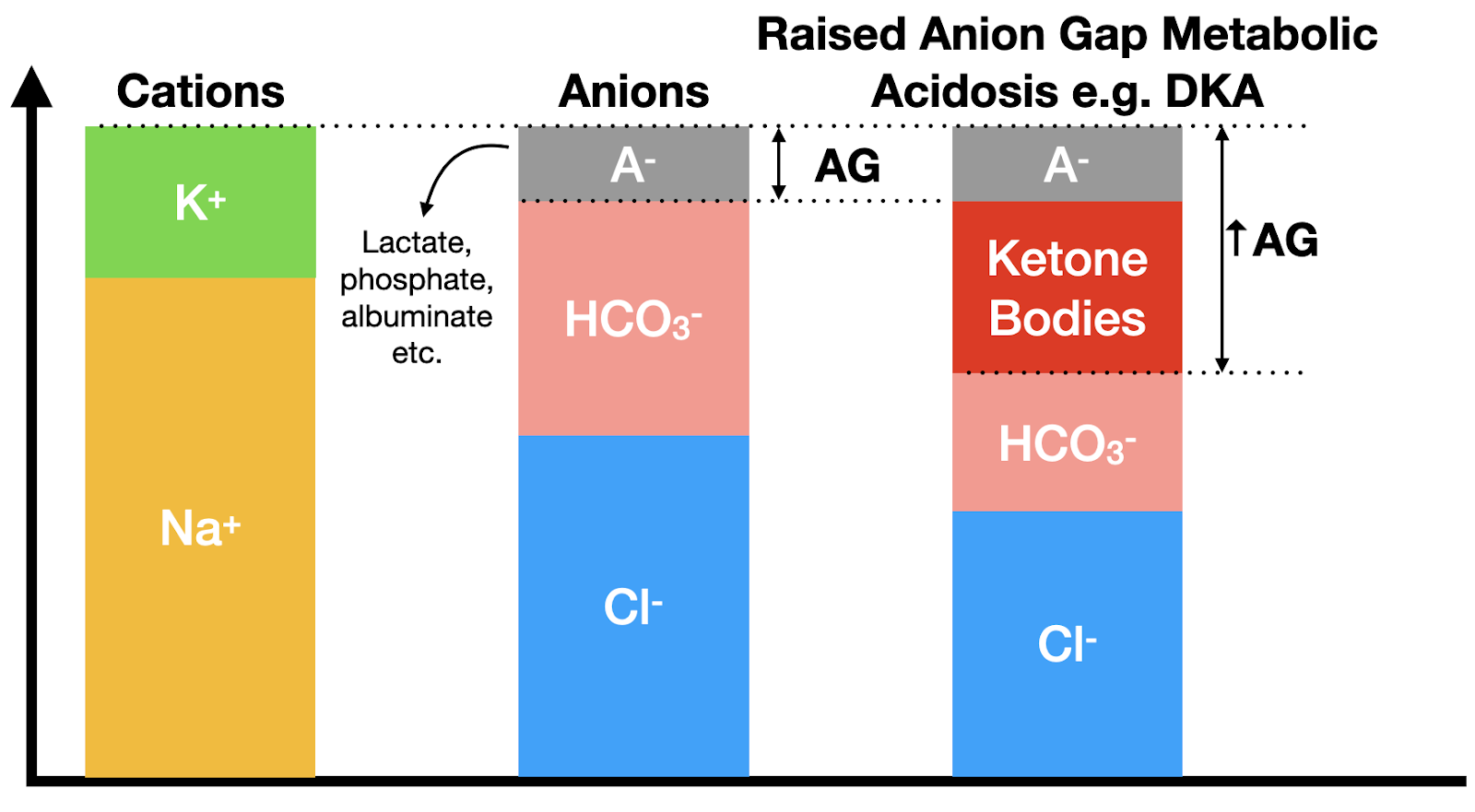
- Calculate the anion gap: [Na+] + [K+] - ([Cl‐] + [HCO3‐])
- If raised (N.R. 10-16mmol/L), this suggests that an additional acid is present:
- Intake of exogenous acid: e.g. salicylate (e.g. aspirin) poisoning
- If the anion gap is normal, this suggests an electrolyte derangement is the primary cause e.g. renal tubular acidosis.
Increased production of endogenous acids or decreased acid excretion: e.g. ketoacidosis (DKA)
- What are the other values like?
- Electrolytes
- Lactate - quick way to identify a potential cause of a raise anion gap
- Glucose
- Haemoglobin (Hb) - notoriously inaccurate on ABGs!
- Methaemoglobin (MetHb) - oxidised form of Hb caused by errors of metabolism or by exposure to toxins such as nitrates.
- Carbon Monoxide (CO) - in city dwellers or smokers levels can be raised up to 10% but a level >10% indicates poisoning
- Determine the Cause: