ECG measures small extracellular currents at the body surface
These dipoles are the result of, but not equal to, myocardial action potentials
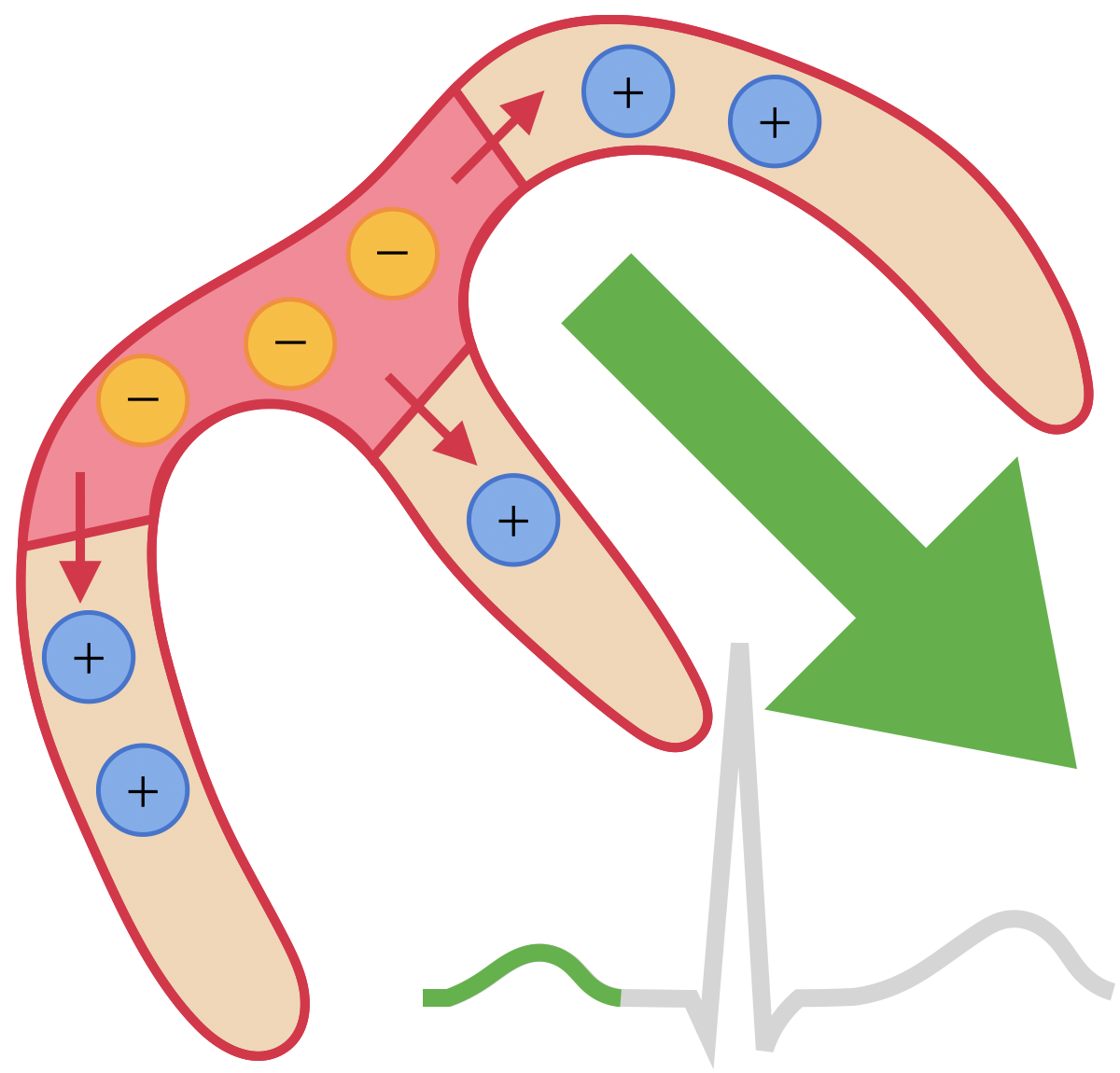
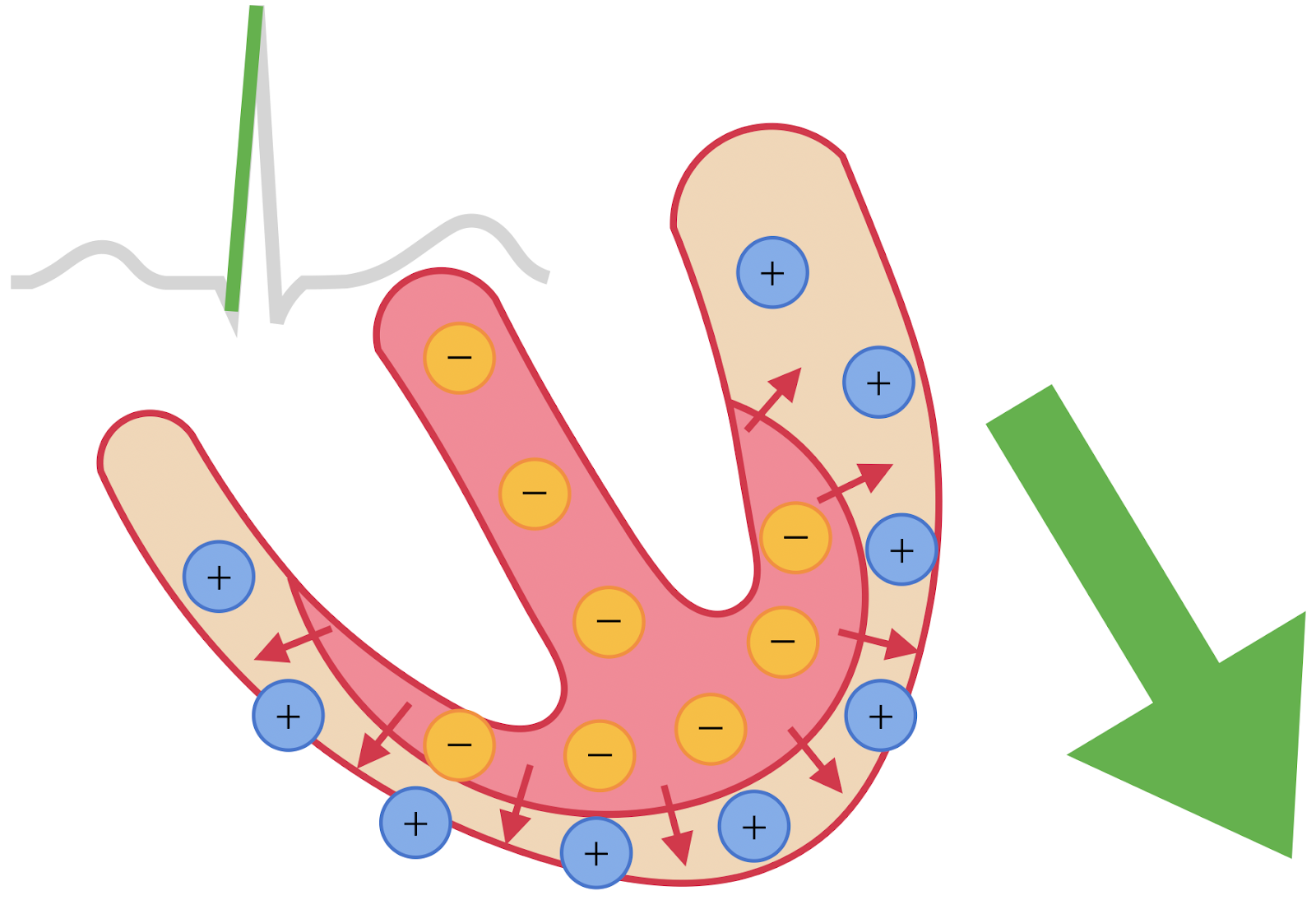
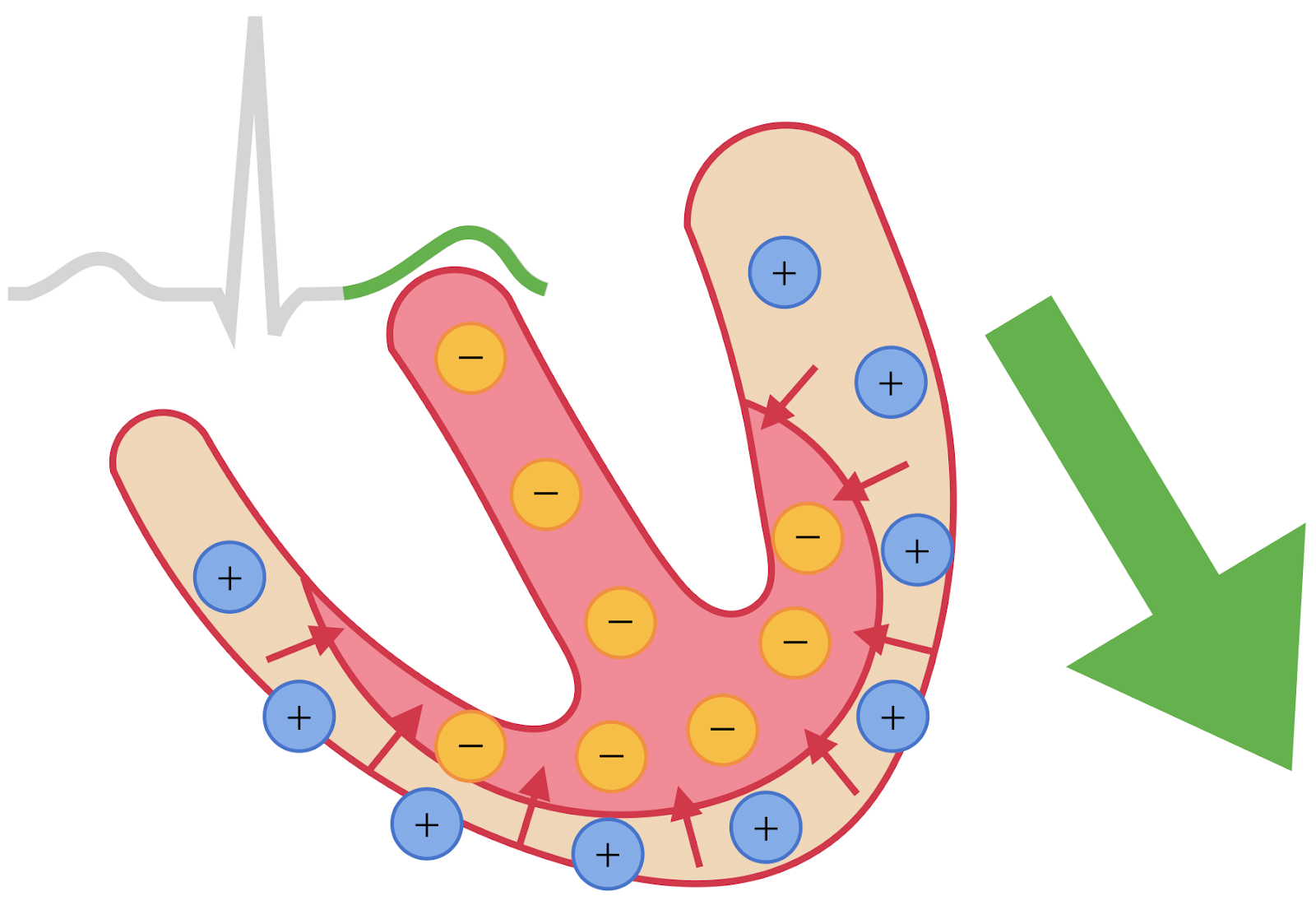
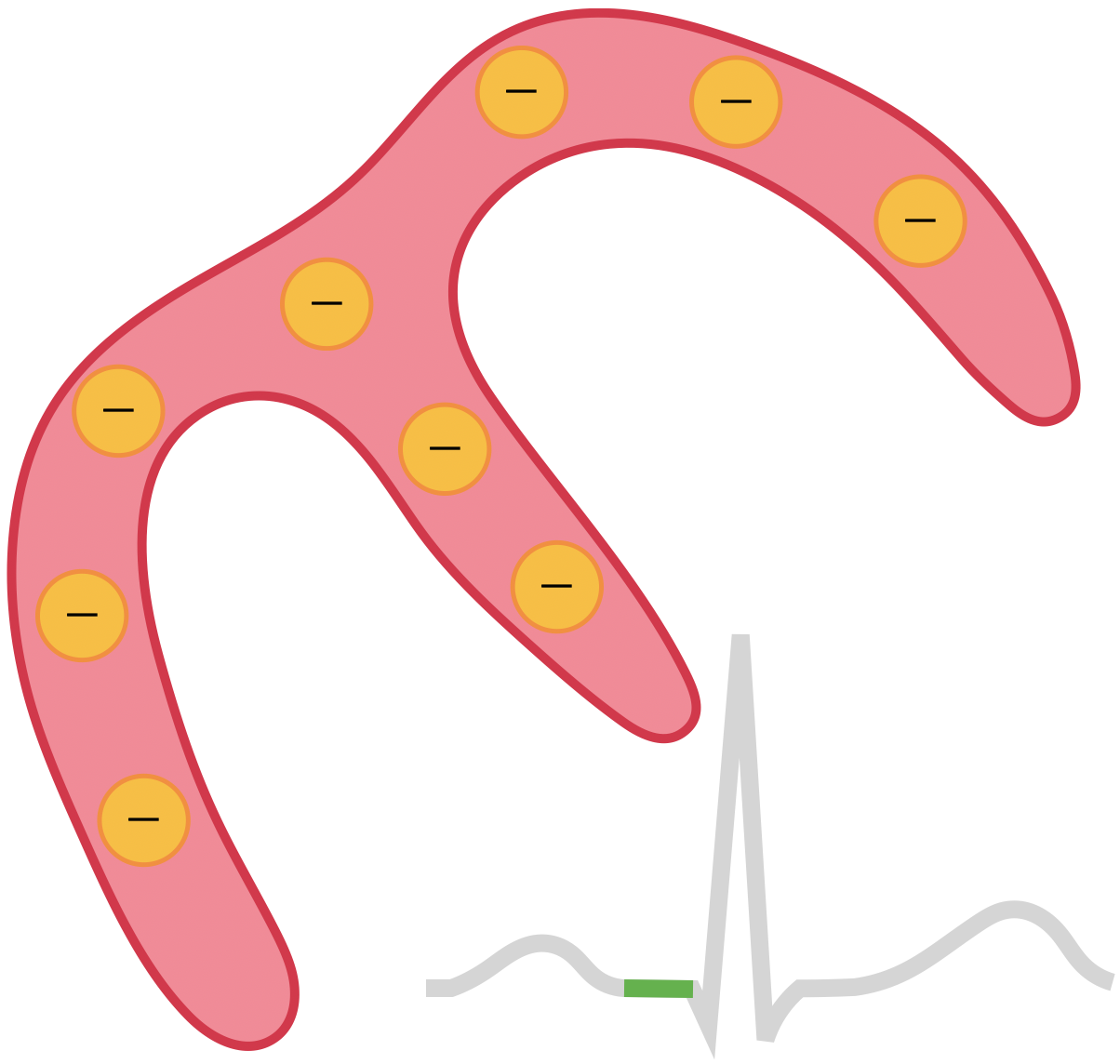
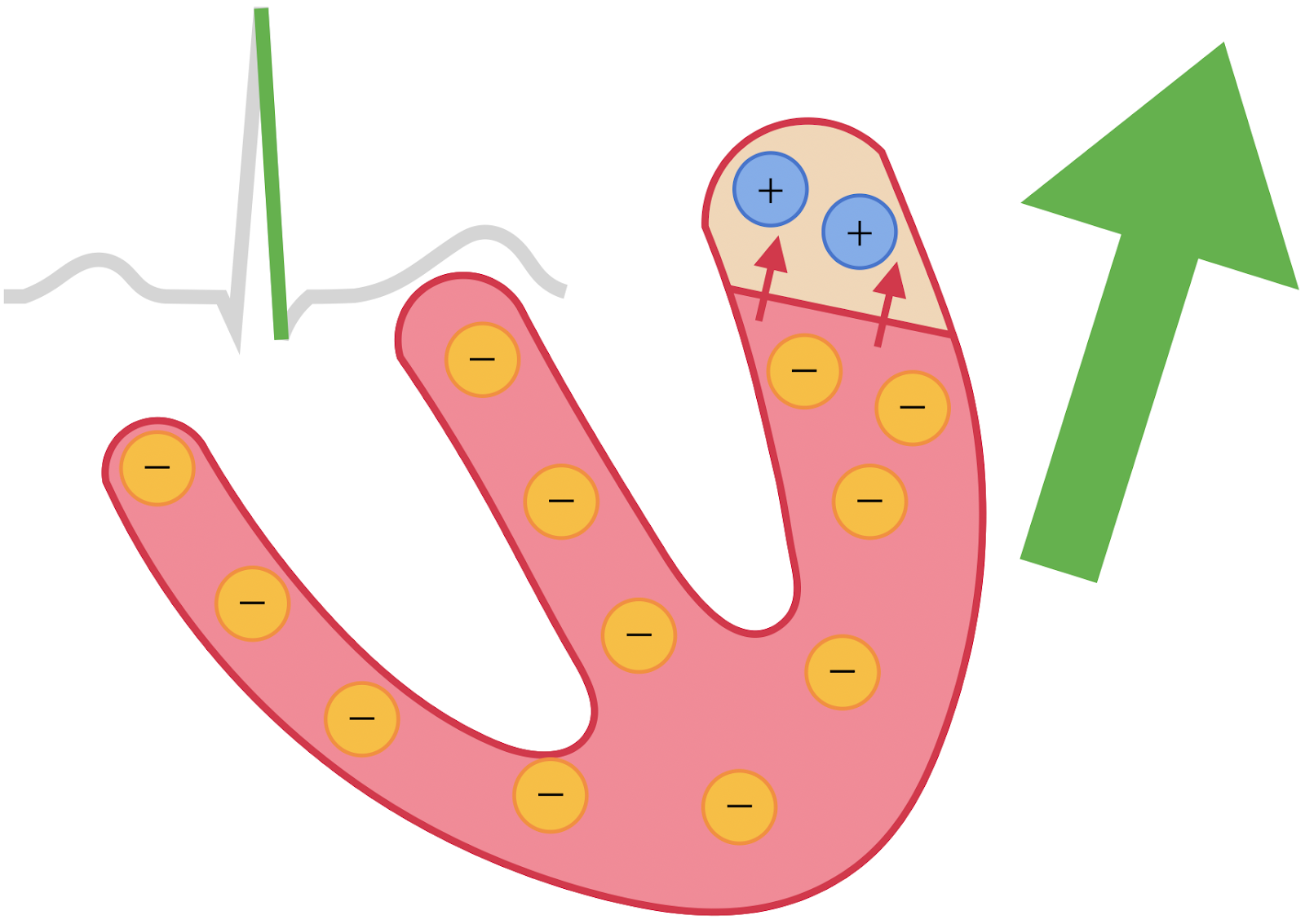
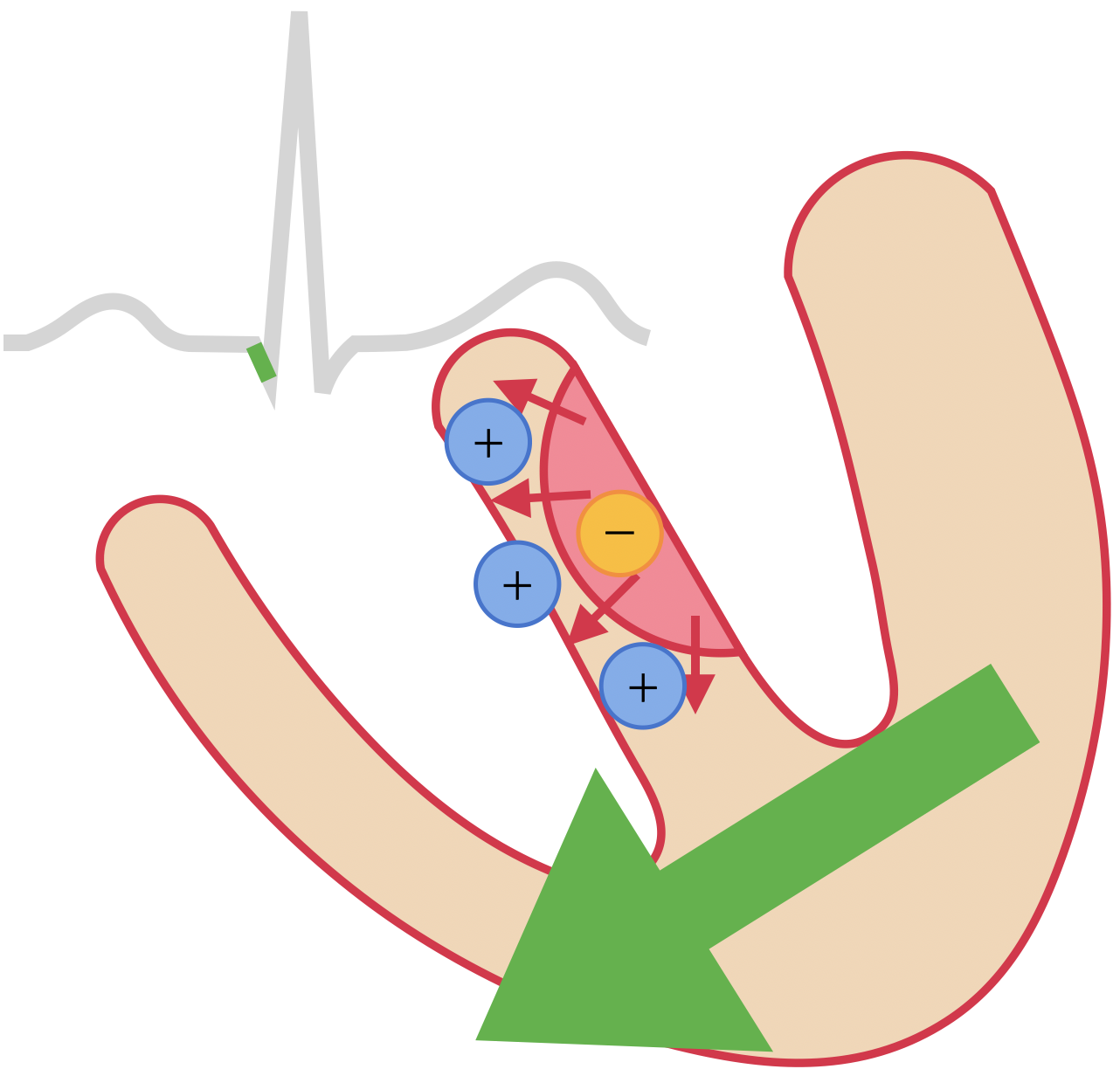
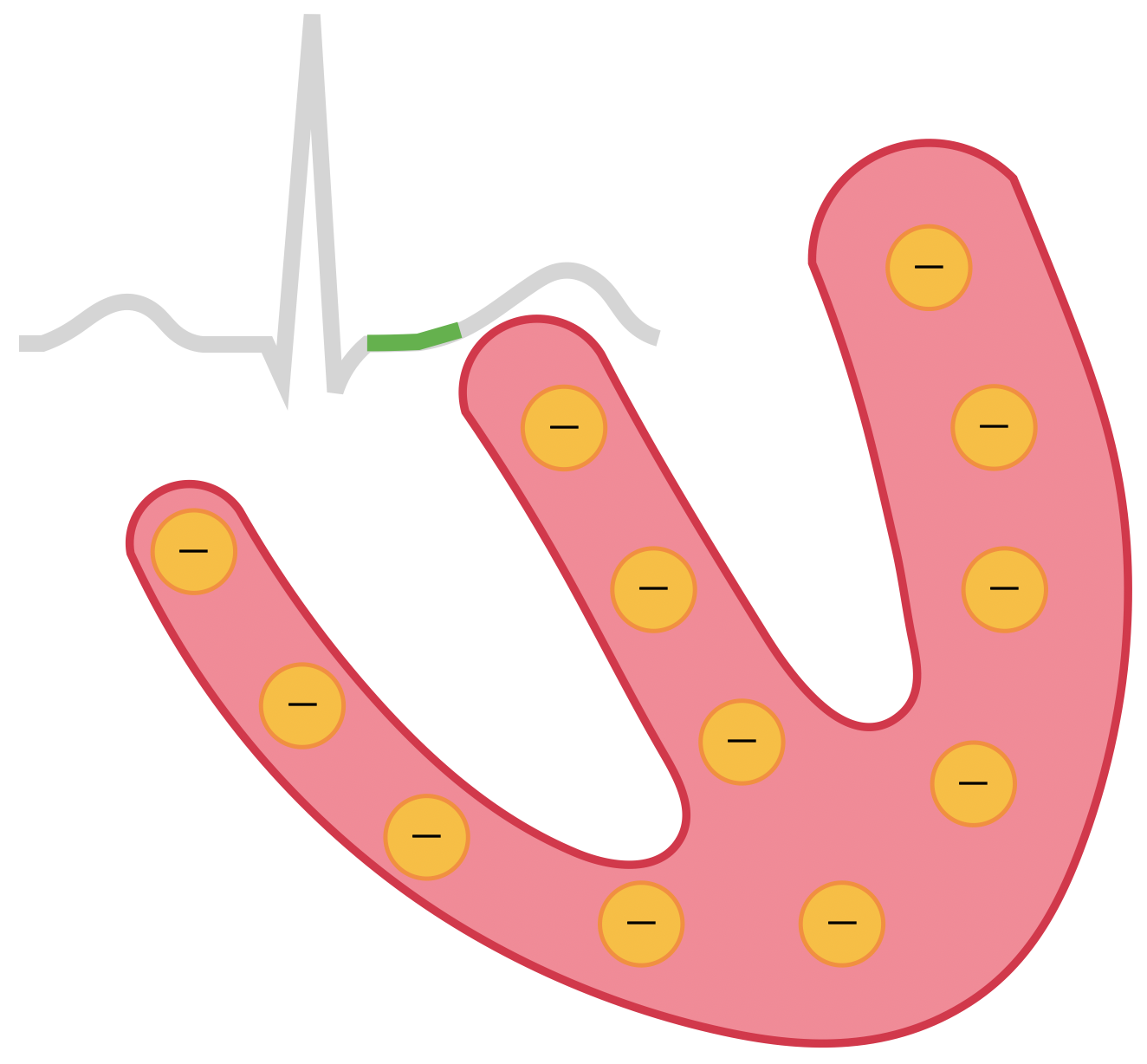
Movement of negative extracellular charge towards (or positive away) from an electrode gives a positive deflection.
Dipoles are vectorial: have magnitude and direction
N.B. An electrical axis measuring perpendicular to a dipole will register no signal.
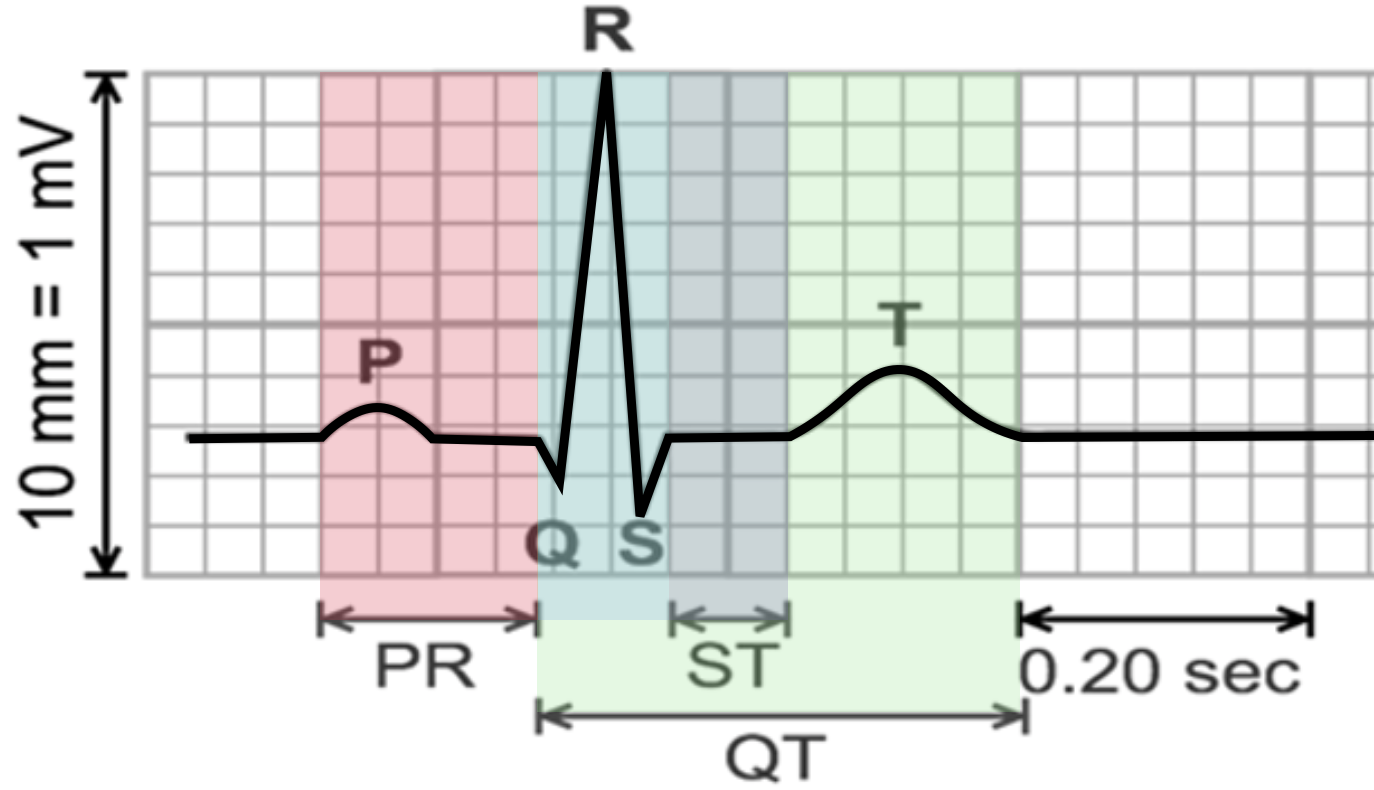
What do the waves represent?
P wave
Atrial Depolarisation
R wave
Ventricular Depolarisation
PR interval
AV node delay
S wave
Left Ventricular Depolarisation
T wave
Ventricular Repolarisation
Q wave
Septal Depolarisation
ST segment
Isoelectric Depolarised Ventricles
QT interval
Duration of ventricular depol + repol
RR interval
Duration of one ventricular cycle
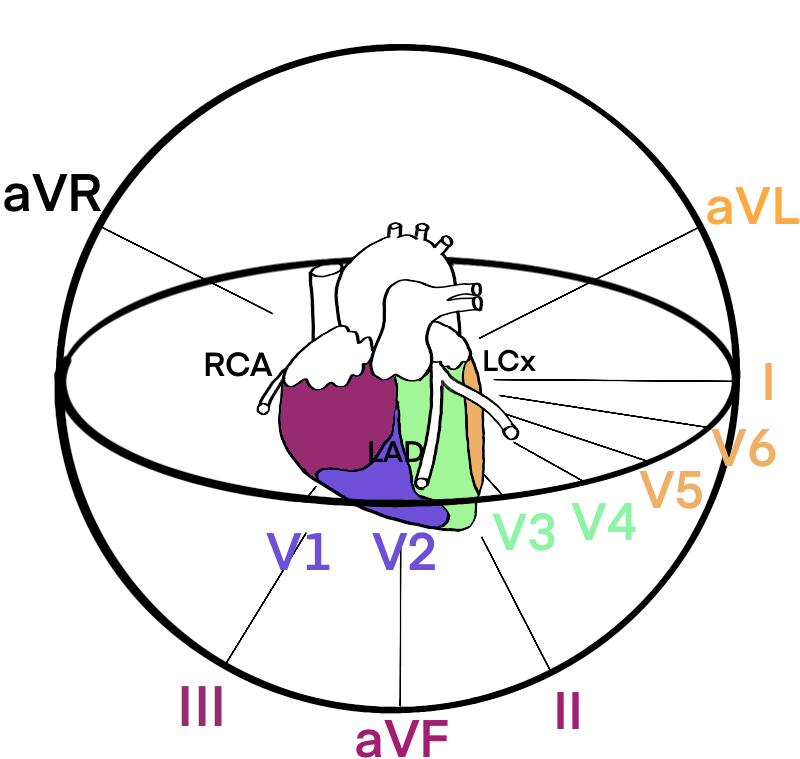
Electrode Placement and Lead Distribution
Leads measure the potential difference (voltage) across the axis formed between two electrodes - e.g. lead I is the difference between the electrodes on the right and left arms; it ‘looks across’ the heart. A typical ECG will have 12 leads generated from 9 electrodes (+ ground) in 2 planes:
N.B. the unipolar leads are ‘virtual’ leads calculated from the other leads
Transverse: 6 precordial leads (V1-V6)
This gives a 3D view of the heart which can be very helpful in localising ischaemia or an MI.
I lateral
aVR
V1 septal
V4 anterior
II inferior
aVL lateral
V2 septal
V5 lateral
III inferior
aVF inferior
V3 anterior
V6 lateral
Rhythm Strip (normally lead II)
INTERPRETING THE ECG
Clinical Context
Patient name, DoB, time ECG taken. Previous ECG to compare?
Technical details:
Speed (25mm/s)
Voltage (10mm/mV = 2 big squares)
Any abnormal lead placement?
(Ventricular) Rate
If regular:
Divide 300 by # big squares between adjacent QRS complexes
Divide 1500 by # small squares
If irregular:
Count #complexes in rhythm strip and x6
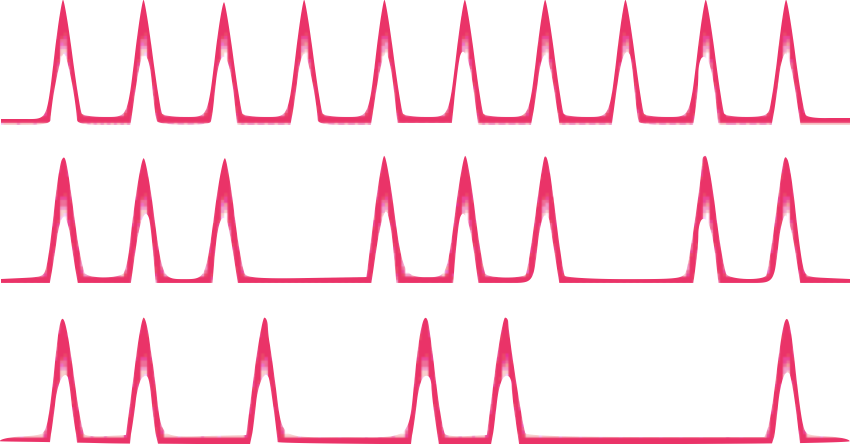
Rhythm
Regular or Irregular?
If irregular:
Regularly Irregular or
Irregularly Irregular
P wave before each QRS? If not what ratio?
Pacing spikes?
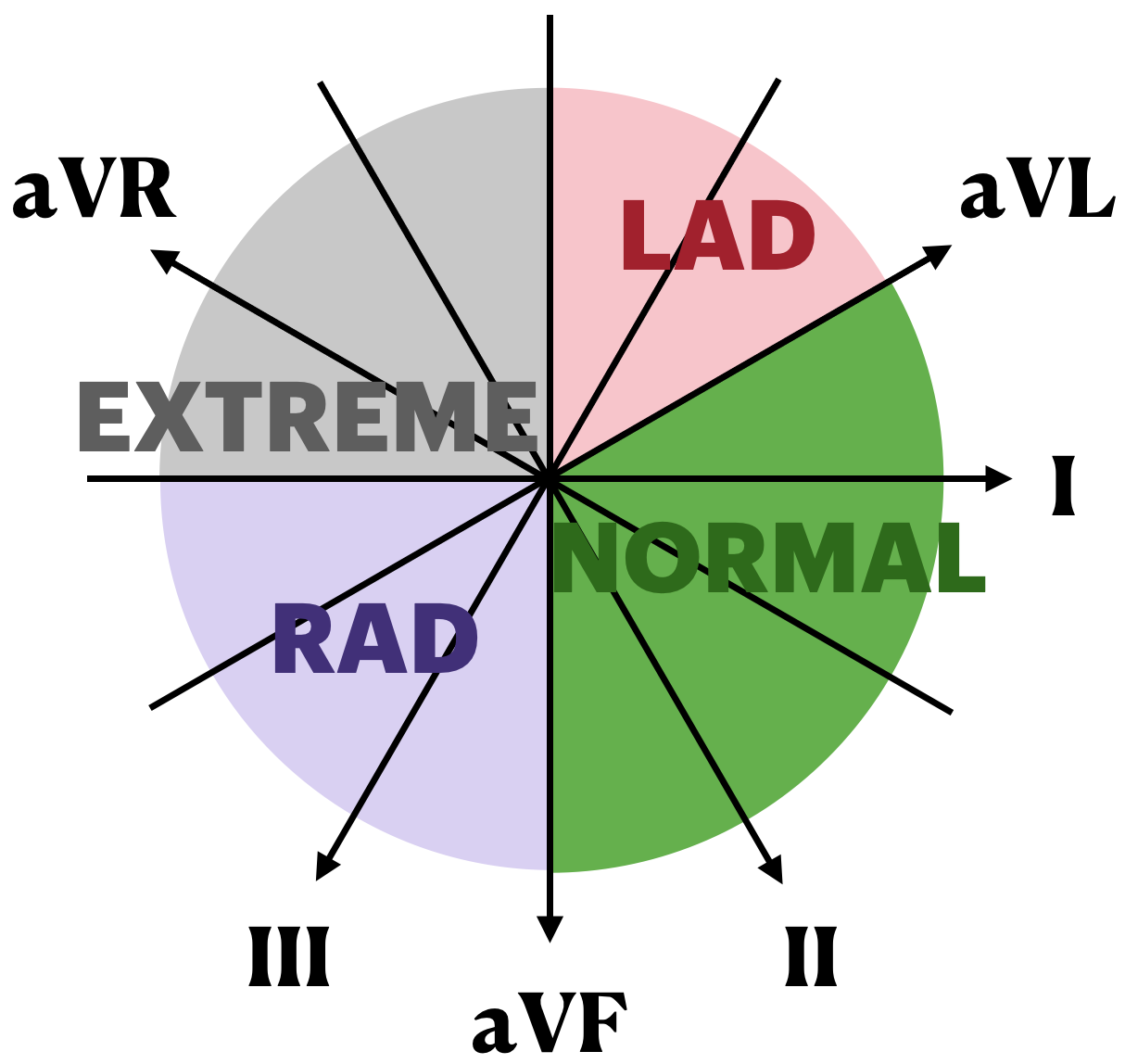
(QRS) Axis
Average direction of electrical activity during ventricular depolarisation. Deviation gives insight into chamberenlargement, conduction abnormalities and some arrhythmias.
Look at the net direction of the QRS in leads I and II:
Normal is positive in lead I and II
Left axis deviation is positive in I and negative in II (left is leaving)
Seen in left anterior hemiblock, LVH and inferior MI
Right axis deviation is positive in II and negative in I (right is reaching)
Seen in right heart strain and RVH
P wave
Normal - <3 small squares (0.12s), <2.5ss high
Positive in II, biphasic in V1
Absent + Irregularly Irregular → AFib
Sawtooth + 2:1 (or 3:1/4:1)ratio with QRS → Atrial Flutter
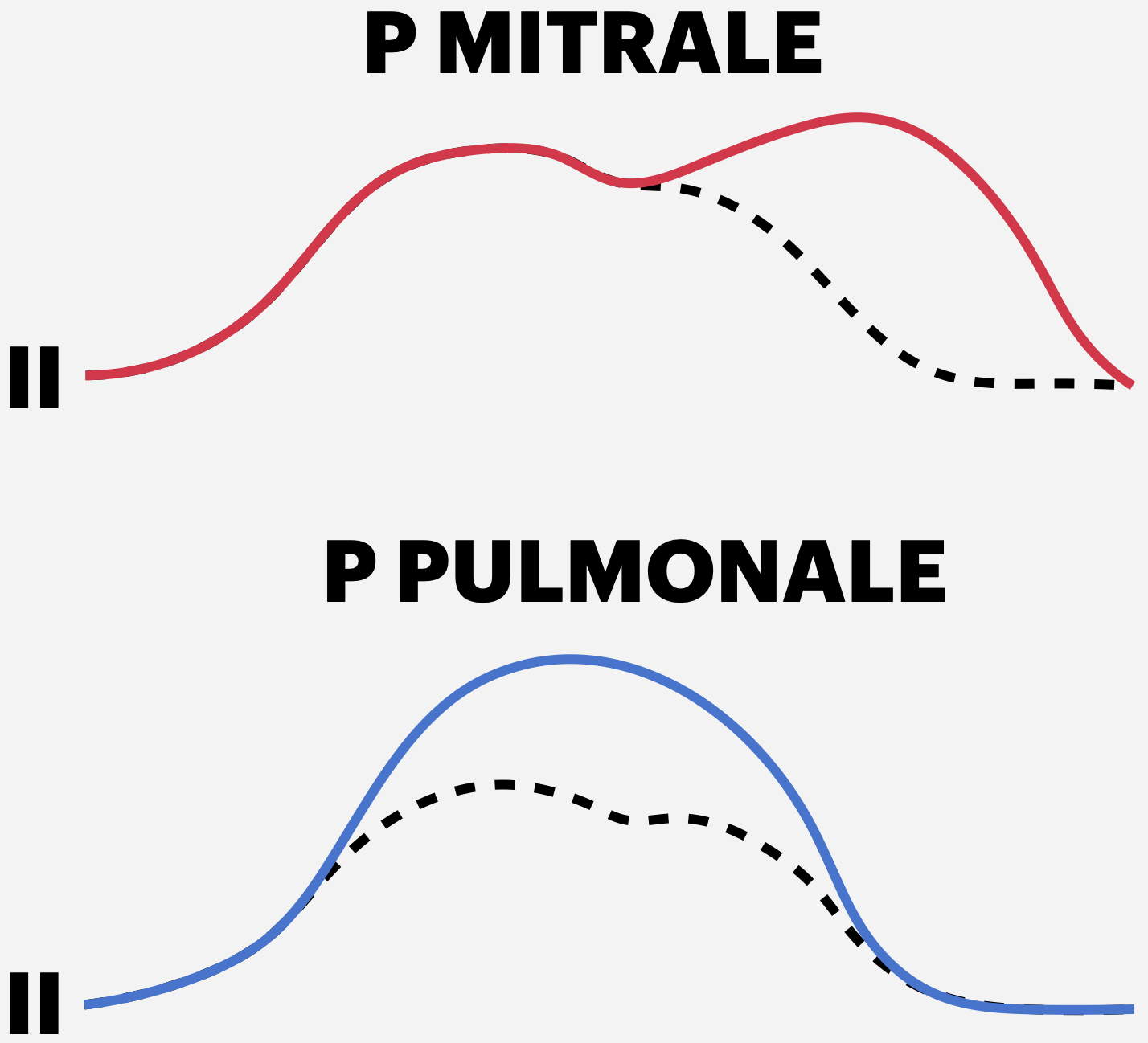
Morphology:
Bifid (= P mitrale → left atrial hypertrophy
Peaked (= P pulmonale → right atrial hypertrophy)
PR interval
P always followed by QRS? No = heart block:
1st degree = prolonged PR interval (>3 small sq/0.12s)
2nd degree
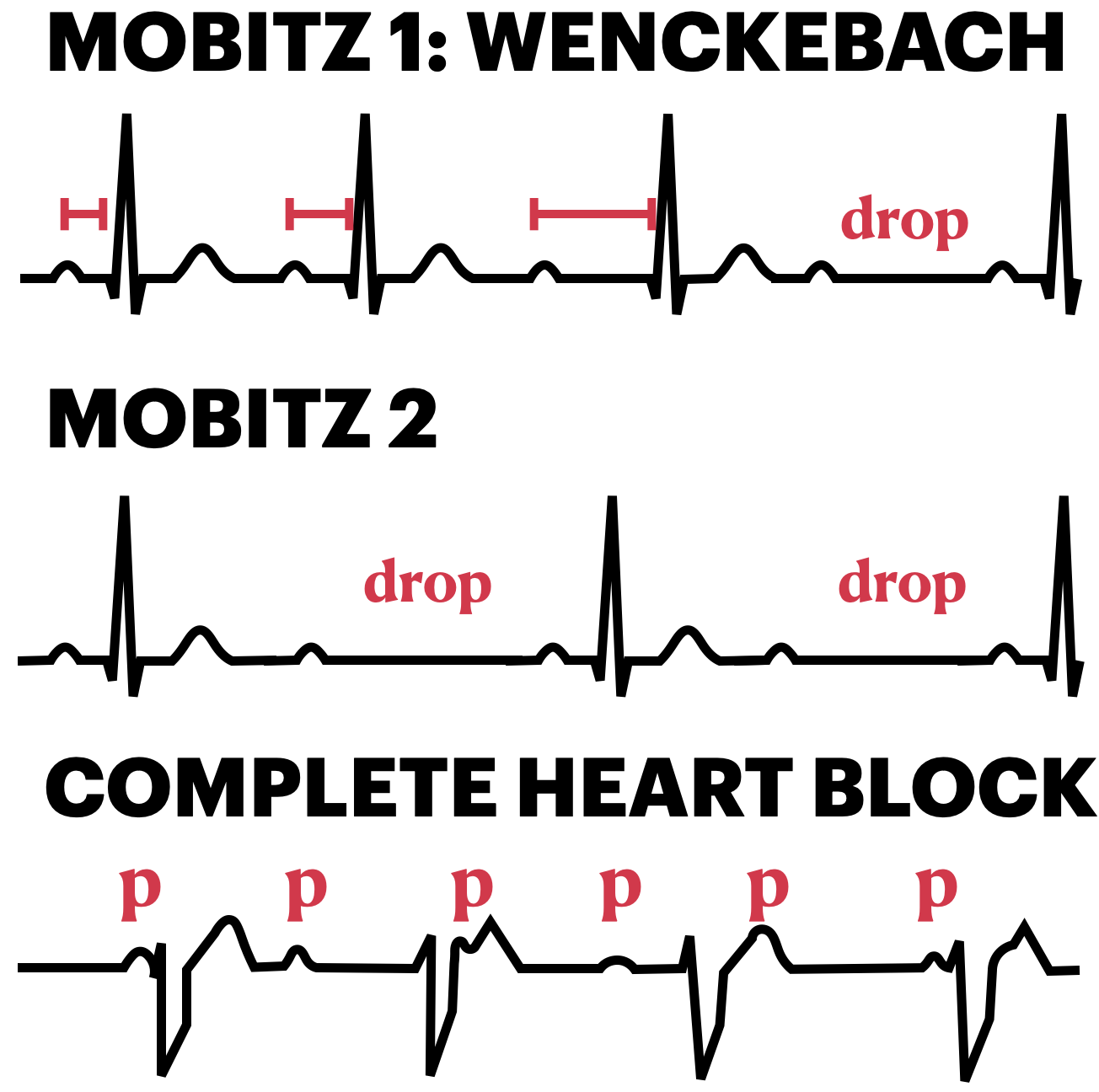
Mobitz type 1 (Wenckebach): progressive lengthening of PR interval eventually resulting in a dropped beat
Mobitz type 2: intermittent non-conductions of P waves, not preceded by PR lengthening (what’s the ratio? E.g. 2:1)
3rd degree (complete) heart block: complete dissociation between P waves and QRS
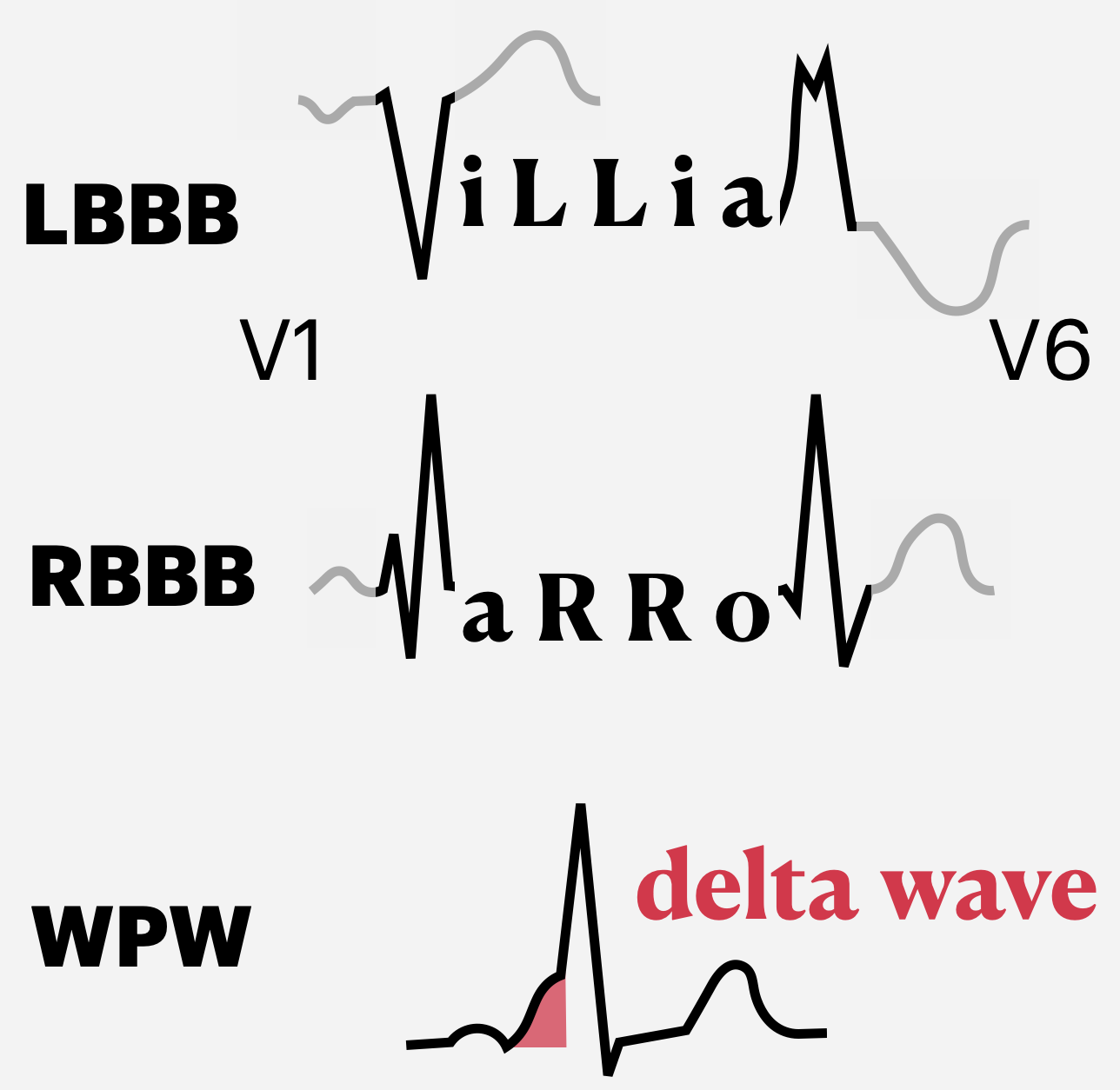
QRS complex
Duration: <3 small sq (0.12s), broad = conduction abnormality: