TO START |
W2I2P4E2 | Wash your hands Wear appropriate PPE Introduce yourself and check patient’s Identity Permission: ‘Would it be alright if I examined your legs and stomach?’ Privacy: Ensure curtains to the bay are closed Pain: “Are you in any pain at all?” Position: Patient lying flat in bed Exposure: Trouser and socks off with a sheet across hips
|
INSPECTION |
Surroundings
| Monitoring - ECG, pulse oximetry Treatments - IV access, fluids, compression stockings/devices, anti-coagulant medication, dressings Paraphernalia - walking aids, wheelchair, cigarettes
|
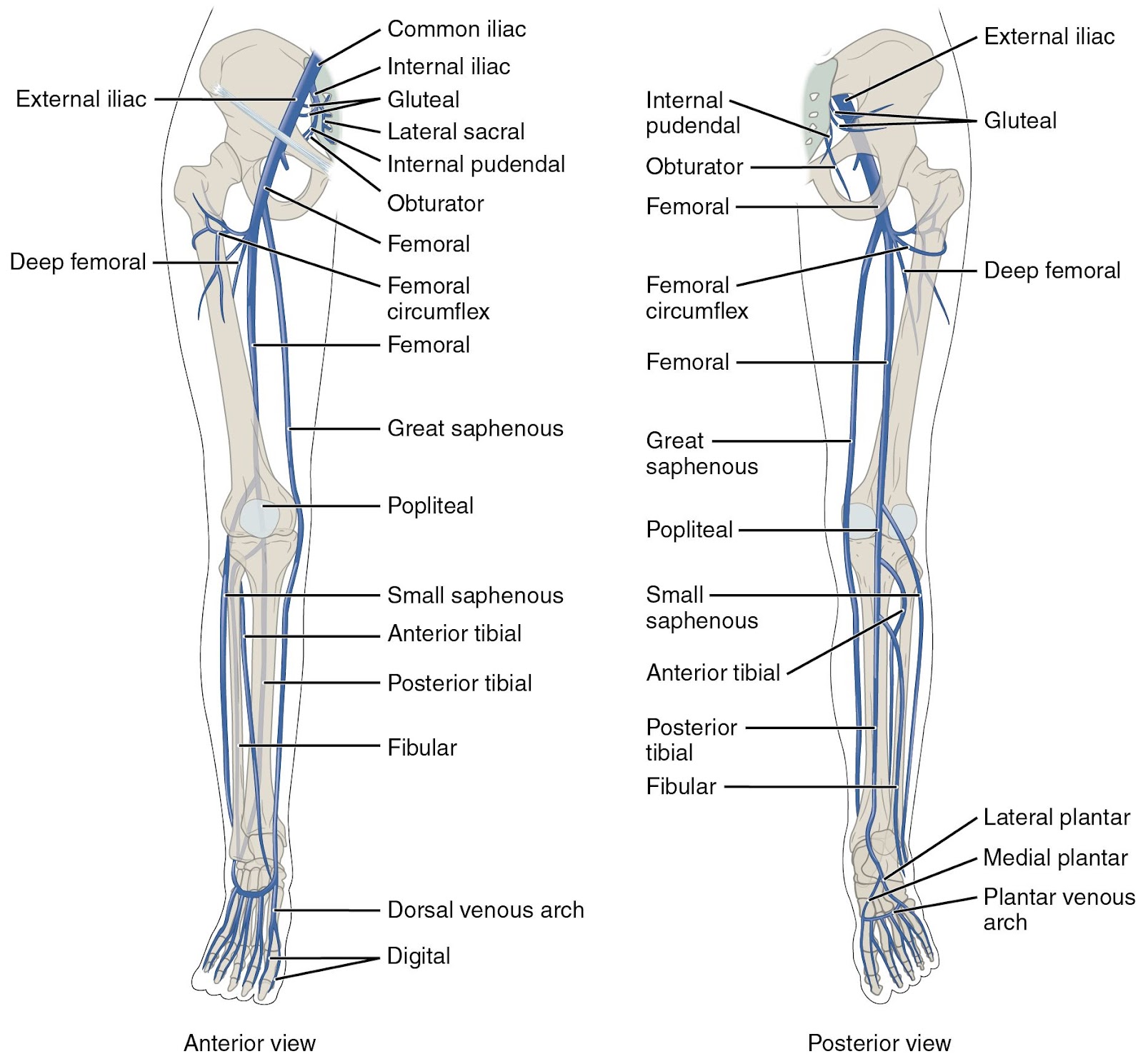
Legs | Inspect the entire course of the superficial veins of the legs. Long Saphenous Vein (LSV): runs up the medial aspect of the leg to join the femoral vein at the sapheno-femoral junction. Inspect with the leg externally rotated. Short Saphenous Vein (SSV): runs posteriorly behind the lateral malleolus and joins the popliteal vein. Inspect leg from the back. Sapheno-Femoral Junction (SFJ): found 2.5cm below and lateral to the pubic tubercle. Saphena varix = dilatation of the saphenous vein at the SFJ and appears as a blue-tinged bulge, which disappears on lying flat and has a cough impulse.
|
Signs of Chronic Venous Disease | Venous disease typically manifests in the ‘gaiter area’ (lower shins) Lipodermatosclerosis: skin is hard, fibrotic (indurated), blue/purple/black/red. Legs are ‘inverted champagne bottle’ shaped (narrowing to a point distally). Atrophie Blanche: white spots on a pigmented background of haemosiderin staining dilated capillaries. Venous Eczema: dermatitis which can blister/ulcerate. Venulectasia: dilated subdermal veins lead to corona phlebectatica (red-pink hue) above the ankle. Smaller in size to varicose veins. Venous Ulcers: typically over shins in the distribution of LSV and SSV territory (cf arterial ulcers over pressure points), with sloping edges and a sloughy appearance. Medial ulcer = LSV, lateral ulcer = SSV. Oedema, Thrombophlebitis, Scarring from healed ulcers.
|
Signs of DVT |
|
PALPATION |
General | Temperature: use the backs of your hand to compare both legs, feeling up the length of the legs to detect any changes in temperate. Pitting Oedema: how far does it extend? Push your thumb into the patient’s legs on bony prominences, going higher until oedema stops. Calf Tenderness and Warmth: tender, red, swollen calf is a DVT until proven otherwise.
|
LSV, SSV and SFJ
| Palpate along the course of the LSV and SSV, looking for: Varicosities (dilatations) Thromboses (thickened, firm veins) Thrombophlebitis (red, tender, cord-like veins. DVT in 40%)
Cough Impulse over SFJ: saphenovarix? Palpable thrill = incompetent SFJ valves.
|
PERCUSSION |
Tap Test | |
AUSCULTATION |
|
SPECIAL TESTS |
Trendelenberg Test | Ask the patient to lie supine and raise their leg to 45° (rest it on your shoulder). Empty the leg veins by massaging distally to proximally. Firmly apply pressure with two fingers over the SFJ and ask the patient to stand. If the varicose veins immediately refill, valve incompetence is below the SFJ. If the varicose veins only refill after releasing the pressure from the SFJ, this indicates valve incompetence at the level of the SFJ (a positive test).
|
Tourniquet Test | Begin the same as the Trendelenberg test, but apply a tourniquet to the proximal thigh between the SFJ and the mid-thigh perforator. Ask the patient to stand. If the varicose veins rapidly refill, the valve incompetence is below the level of the tourniquet. Apply the tourniquet to progressively distal locations until the veins do not rapidly refill, indicating the level of valve incompetence.
With the patient standing, apply a tourniquet just below the knee joint. Ask the patient to flex the knee 10 times and observe the varicose veins. If the varicose veins empty, the valvular incompetence must be above the level of the tourniquet. Rapid refilling implies valve incompetence in the calf. Pain suggests deep venous occlusion and requires a duplex scan.
N.B. offer to do these tests for patients with obvious varicose veins. These tests are uncomfortable for patients and it is unlikely that you will do them. |
TO COMPLETE |
Closure | |
Examinations | Arterial exam: especially ABPI, as the compression stocking used to treat venous congestion are contraindicated in arterial insufficiency. Consider pelvic or abdominal causes for varicose veins eg IVC obstruction secondary to an abdominal mass/lymphadenopathy.
|